
AUTOMATED BREAST PLANNING IN RAYSTATION
For over a decade, intensity modulated radiation therapy (IMRT) has been employed in tangential beam adjuvant breast-conserving treatment. The various simple and advanced forms of intensity modulation have been shown in randomized trials to significantly improve cosmetic results, reduce acute side effects and improve breast dosimetry over non-modulated methods.
Automated breast planning can be used to reduce the time and effort required to create highly individualized tangential breast IMRT treatment plans. It is applicable for most early stage breast cancer patients receiving tangential breast radiation therapy (RT). Integrating automation into routine clinical practice allows the planning process to be highly standardized, while still focusing on personalized cancer care. By using automated methods, centers can more rapidly adopt IMRT and enhance access to the documented potential improvements for breast cancer patients, using technologies that are widely available and already in clinical use.
RAYAUTOBREAST IN RAYSTATION
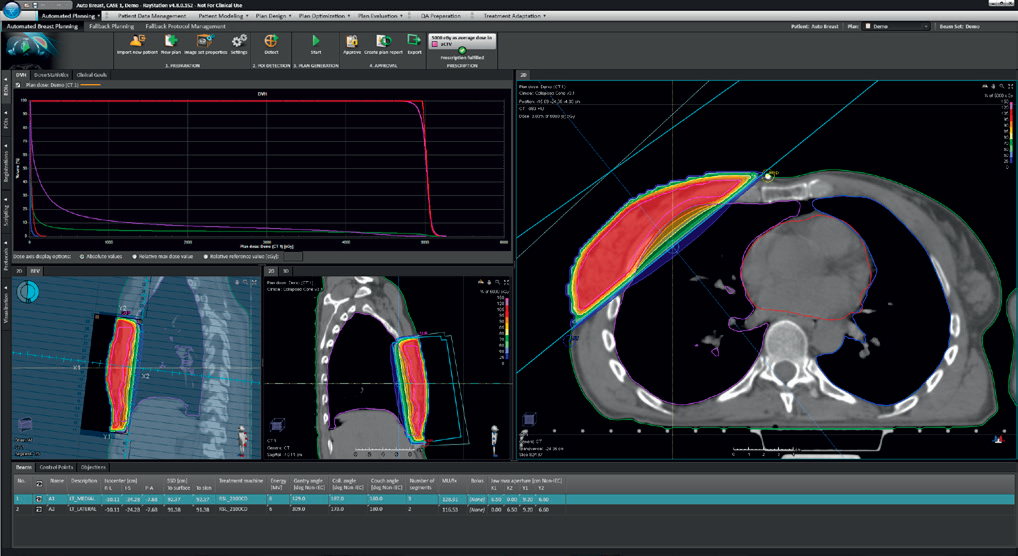
The automated tangential breast treatment planning module in RayStation, rayAutoBreast, is a fully automated treatment planning solution that performs all manual planning tasks including segmentation of all relevant structures, placement of beams, setting IMRT optimization parameters and objectives, dose calculation and automated plan reporting.
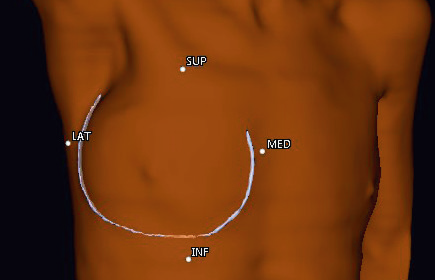
The patient-specific data that drives the algorithm, is captured at the time of simulation through the use of wires and markers. Specific marker placement is required and captured during CT scanning. A wire is placed around the breast tissue or along the chest wall together with with four markers denoting the superior, inferior, lateral and medial margins.
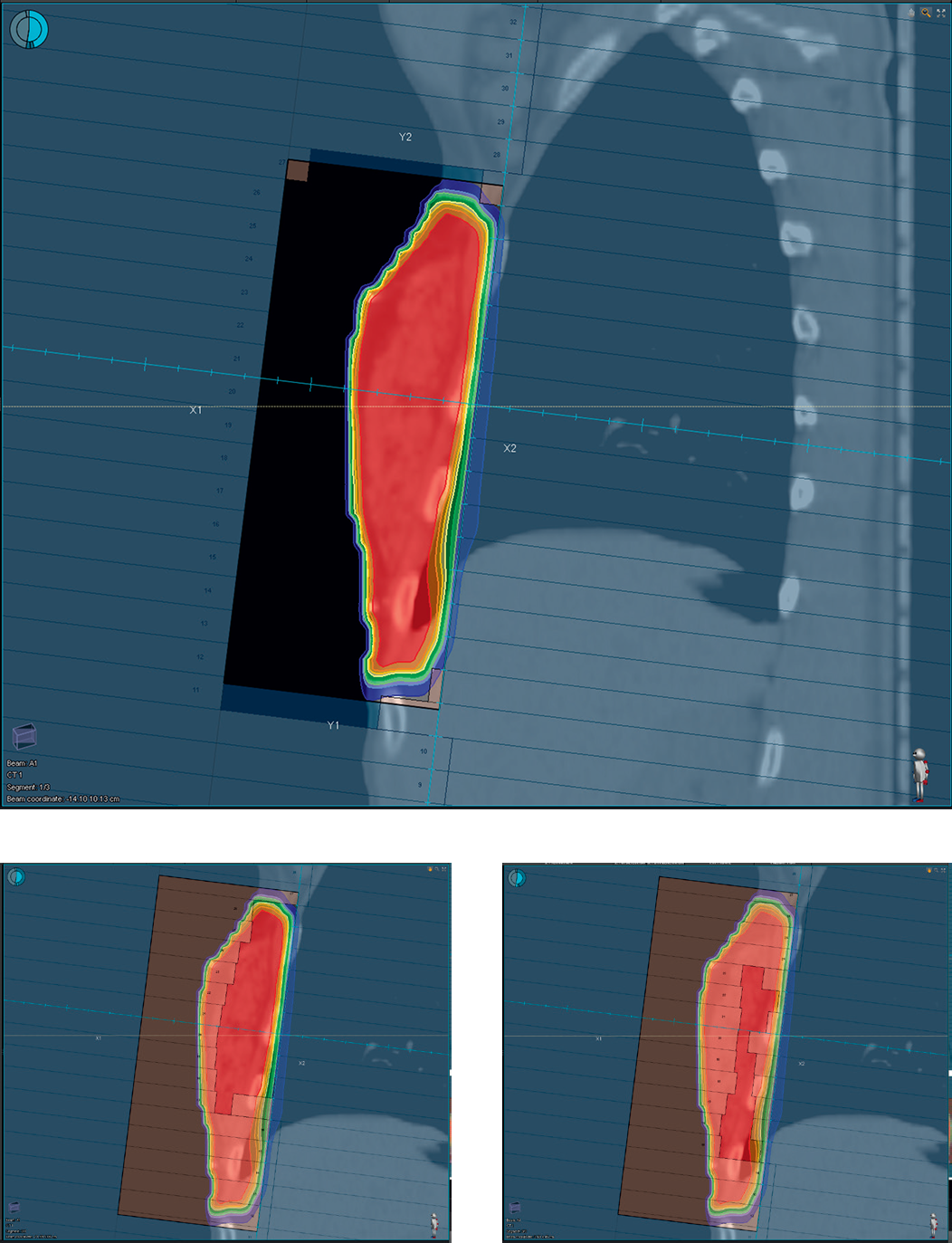
Heuristic optimization relies on features such as the lung, heart, breast/chest wall, and seroma cavity (provided it is delineated) to place treatment beams. The method generates robust treatment plans with simple modulation by minimizing the number of segments for modulation and by automatically producing large segments that cover the entire breast/chest wall volume and include “flash” that is prospectively optimized. Accordingly, the methodology forces large, highly weighted segments to be generated and prospectively optimized thus eliminating any manual manipulation once the optimization is complete. Total calculation time for all planning steps is in the order of minutes.
The module allows the user to specify clinical objectives instead of technical or dose-volume goals. Since the beam geometry and modulation are the most important consideration in tangential breast plans, the user can tailor how the automated algorithm prioritizes competing clinical objectives. Default settings provide the user with a fully automated solution that will apply for the majority of patients. However, advanced settings are available for the user to specify how the automated algorithm prioritizes the clinical objectives.
For example, the user can:
• Specify the acceptable amount of lung volume in the treatment beams
• Specify the margin between the beam and seroma cavity
• Specify the beam shielding for normal tissues
• Constrain the limits in which beams are angled
• Apply geometric beam adjustments depending on breast size/chest wall and seroma cavity location.
PRESCRIBED AND DATA-DRIVEN AUTOMATED PLANNING METHOD
Tangential breast IMRT should be simple to implement and execute; therefore, the role of automation here is to provide standardization and to eliminate any technical complexity while still achieving the prescribed clinical objectives. The methodology presented is very specific to breast treatment planning as we have effectively captured the human decision-making for breast IMRT planning by developing both prescribed and data-driven rules and encoding these rules so that they can be implemented as an automated approach. Other automated planning methods based on data-driven concepts are not well suited to the breast radiation therapy problem. Breast radiation therapy is highly dependent on beam geometry and the problem of placing beams is highly constrained. Most automated planning methods are focused on dose-volume objectives with beam geometry as a secondary consideration. Such conventional commercial automated planning algorithms do not provide clinically relevant solutions “out of the box” and require user intervention to overcome these limitations. The concept of encoding rules and specifying clinical objectives with associated priorities using the breast module is an efficient way to automate the tangential beam IMRT breast planning process while maintaining the properties and quality of the manual methodology.
CLINICAL EVALUATION AT PRINCESS MARGARET CANCER CENTRE
Automated breast radiation therapy has been used at the Princess Margaret Cancer Centre since June 2009, with more than 3,000 patients receiving treatment. Two published papers have detailed automated planning as follows:
1) preliminary method paper, showing feasibility of the approach in a retrospective study [1], and
2) a prospective clinical implementation paper showing results for more than 1,600 patients over 3 years [2].
The clinical implementation work showed decreases in the number of overall plans rejected and number of plan rejections due to planning errors during the conventional quality control treatment planning process or the multi-disciplinary case review rounds. This was because automation was added into the breast radiation therapy planning process. The method provides a high level of standardization and eliminates all need to specify technical parameters for planning.
The automated planning method is available in RayStation, incorporating all the same features that are outlined in the clinical implementation paper.
CONCLUSION
The clinical use of automated tools for complete tangential breast planning has been established and can be used on a large scale. With RayStation’s automated breast planning module, rayAutoBreast, institutions can add efficiency, standardization and quality to the planning process for breast radiation therapy. The automated planning tools can readily be incorporated into an institution’s planning process and provide a rapid planning solution with minimal overhead and resource utilization.
REFERENCES:
[1] Purdie TG, Dinniwell RE, Fyles A, et al. Automation and Intensity Modulated Radiation Therapy for Individualized High-Quality Tangent Breast Treatment Plans. Int. J. Radiat. Oncol. Biol. Phys. 90:688–695, 2014.
[2] Purdie TG, Dinniwell RE, Letourneau D, et al. Automated planning of tangential breast intensity-modulated radiotherapy using heuristic optimization. Int. J. Radiat. Oncol. Biol. Phys. 81:575–83, 2011.
For more information or to see a demo, contact sales@raysearchlabs.com