
BIOLOGICAL OPTIMIZATION AND EVALUATION IN RAYSTATION
The clinical goals of treatment planning are usually stated indirectly as prescribed dose levels to the tumor and limiting dose criteria to the organs at risk. These dose levels are decided with some expected clinical outcome in mind, and they relate to some specific fractionation schedule. If the daily treatments of an individual patient for some reason deviate from the intended ones, the delivered total dose is no longer a predictor of the clinical outcome.
To fully understand the effects of a treatment plan, the time of delivery of each fraction, the dose per fraction, the treatment modality and the number of fractions must be considered. To further complicate matters, different tissues respond differently to radiation. Some cell types are more radiosensitive than others and some organs are more sensitive to hotspots than others. The biological tools in RayStation can be used to explore the biological effects of such non-standard treatments.
BIOLOGICAL EVALUATION
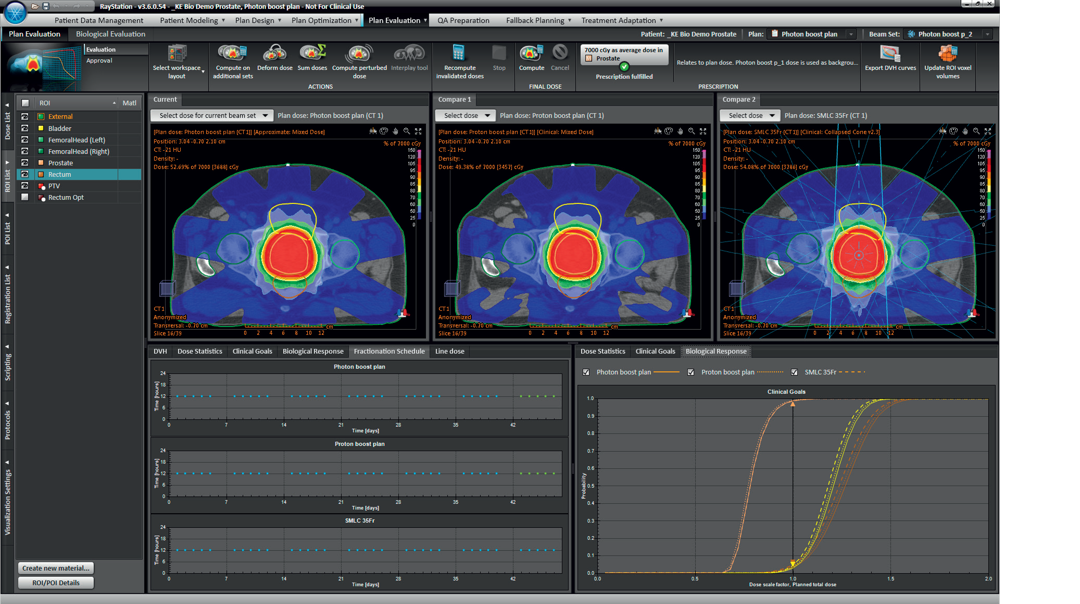
The philosophy is to use the biological models to reveal effects that are difficult to understand from the dose distribution alone and to make the biological evaluation result as transparent as possible. For this purpose, the biological tools are not isolated in a new biological plan comparison module, but instead integrated in the existing plan evaluation module so that the physical properties of the plan can easily be investigated if unexpected differences in the biological response are observed between different plans. In addition to the biological plan comparison in the Plan Evaluation module, there is a Biological Evaluation module dedicated to the exploration of the biological effects of altering the fractionation schedule of a single treatment plan.
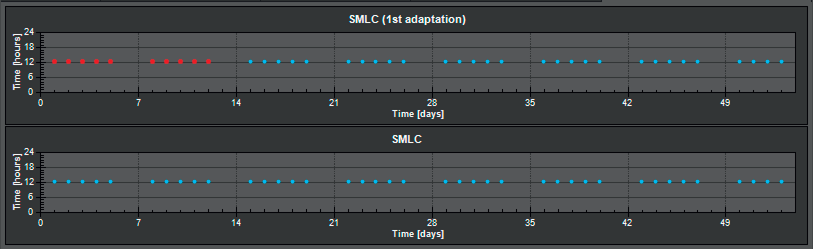
It is possible to compare the Tumor Control Probability (TCP) and Normal Tissue Complication Probability (NTCP) values, and to investigate the biological response curves to see how robust the plans are to changes in the dose per fraction. The biological progress graph shows how the TCP and NTCP values evolve during the course of the treatment. In addition to the physical dose, the fractionation schedules are displayed. The fractionation schedule of the loaded plan and its alternative schedules can be manually modified by moving fractions in the fractionation schedule view, which enables fractionation customization. The biological effects of modifying the fractionation schedule and scaling the dose per fraction can thus be compared with other treatment plans or a copy of the original plan.
BIOLOGICAL OPTIMIZATION
In physical optimization, the treatment goals are stated indirectly by describing the desired properties of the dose distribution to the tumor volume and the organs at risk. In biological optimization, the problem formulation stays closer to the medical goal. By using biological objectives, the necessary trade-off between tumor control and normal tissue protection is handled by the biological models. If the resulting dose distribution is not satisfactory it can be tuned further by adding dose-volume constraints. It is also possible to keep the traditional dose-volume objectives, and to introduce NTCP constraints on some critical structures only. The number of DVH-objectives defined on a structure can usually be reduced by replacing them with one single NTCP function. Generalized Equivalent Uniform Dose (gEUD) can be used for treatment plan optimization together with the physical dose based optimization functions without any biological license, and can also be used for evaluation purposes in the optimization module.
BIOLOGICAL MODELS
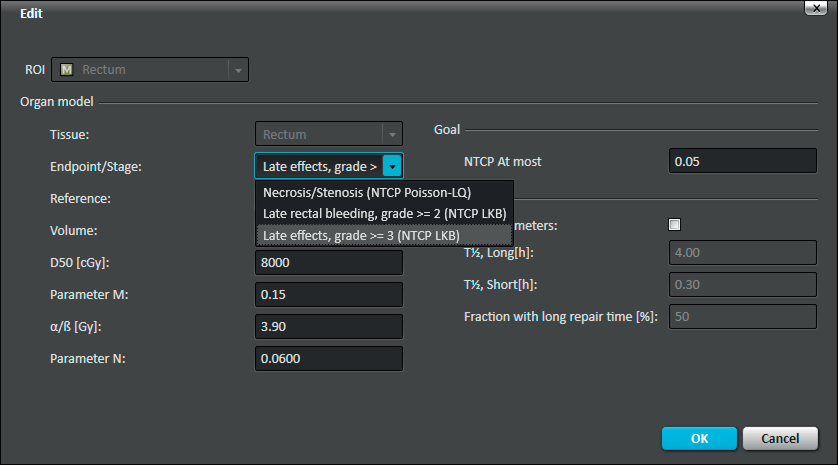
Two of the most common Tumor Control Probability (TCP) and Normal Tissue Complication Probability (NTCP) models, the Poisson- LQ [1,3] and the LKB [2] models, are included in RayStation, together with an editable model parameter database containing default parameters found in the literature. These models can be combined with models for repair and accelerated repopulation. Using the biological model parameter database application, clinic specific TCP and NTCP model parameters can be stored. The parameters can be retrieved from the database by selecting a tissue type, and an endpoint or a stage.
ADAPTIVE TREATMENTS
Due to changing patient geometries in different fractions the cells may experience different doses in each fraction. In an adaptive replanning scenario the total dose may not be enough to understand how the expected clinical outcome of the treatment is affected. The biological models in RayStation can be used to get a hint of how much a plan deviates from the originally planned treatment in terms of biological response. If necessary, TCP and NTCP optimization functions can be added to the original optimization problem formulation to recover the biological effect when reoptimizing the remaining fractions of the treatment.
BOOST PLANS
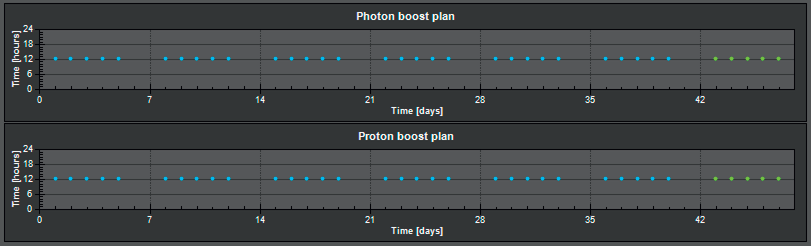
In RayStation it is easy to combine different sub-plans (beamsets) to create a boost plan. The nature of a boost plan is that the dose per fraction is different in the boost fractions compared to the initial fractions. To fully understand the impact of the two different dose distributions it is useful to use biological models for the evaluation, and especially when comparing different boost plans. The biological models can also be used as optimization functions to consider the biological aspects when a boost plan is created.
TREATMENT MODALITY
The biological effect of a treatment depends not only on the time of delivery and the fraction dose distribution, but also on the treatment modality. In RayStation the dose distribution is scaled by a modality specific Relative Biological Effectiveness (RBE) before the TCPs and NTCPs are calculated. The RBE scaling enables comparisons of proton, electron and photon plans, and the calculation of the biological response of photon-proton boost plans.
FUTURE RELEASES
More biology is planned for future releases of RayStation: generalized equivalent uniform dose (gEUD) as clinical goals, visualization of equivalent dose in 2 Gy fractions (EQD2), more elaborate RBE models, brachy models and extended fractionation assessment functionality.
CONCLUSION
RaySearch has since its foundation developed tools for biological evaluation and optimization used both clinically and for research purposes. In RayStation, new graphical tools for biologically based forward planning are combined with proven treatment plan optimization of different planning techniques based on biological models.
REFERENCES
[1] Lind B K, Mavroidis P, Hyödynmaa S and Kappas C, Optimization of the Dose Level for a Given Treatment Plan to Maximize the Complication-free Tumor Cure, Acta Oncologica, 38:787-798, 1999.
[2] Lyman J T, Wolbarst A B, Optimization of radiation therapy, III: A method of assessing complication probabilities from dose-volume histograms, Int. J. Rad. Onc. Biol. Phys., 13:103-109, 1987.
[3] Kallman P, Agren A, Brahme A., Tumour and normal tissue responses to fractionated non-uniform dose delivery. Int. J. Radiat. Biol. Aug; 62(2):249- 262, 1992.
For more information or to see a demo, contact sales@raysearchlabs.com